

Background:
Post-transplant lymphoproliferative disorder (PTLD) is a B-cell proliferation disorder that results from disruption in the physiological mechanisms for proliferation in an immunocompromised host after a solid organ transplant. Our study aims to review the demographic characteristics and clinical outcomes after transplantation. We also aim to study the role of immunosuppression induction therapy, the effect of PTLD on survival, and the effective chemotherapy used for B-cell disorders leading to improved survival.
Methods:
Following the PRISMA guideline, we performed a comprehensive literature search on PubMed, Cochrane Library, Embase, and clinicaltrials.gov from the past decade on May 04, 2020. We used the MeSH terms of organ transplantation and lymphoproliferative disorders. 1741 articles were screened. We excluded all case reports, case series, pre-clinical trials, review articles, and meta-analysis and included three cohort studies and one prospective multicentric study. We extracted the data for baseline characteristics, the reason for transplantation, recipient & donor EBV status, immunosuppression used, type & stage of PTLD, organ system involved, duration between transplant and PTLD diagnosis, treatment, response to therapy, adverse effects of therapy and mortality.
Results:
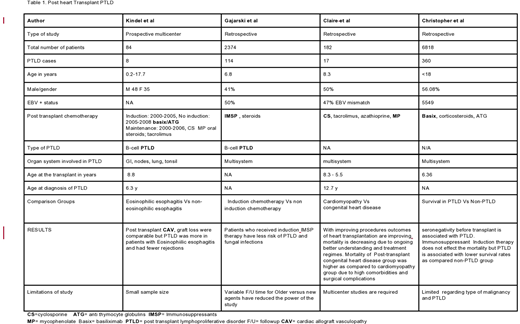
We studied 9617 patients in the included four studies, out of which 499 patients developed PTLD. Data in these studies was collected over the last 20-26 years. Median follow-up of patients since transplant was 3-9 years (average 7.5y). Table 1 The age of the patients ranged from 3-18 years with a male: female gender ratio of 48:52% and around 50% of the patients were seronegative to EBV pretransplant. The following drugs were used for immunosuppression: cyclosporin, tacrolimus, azathioprine, mycophenolate, interleukin 2 receptor antagonist (basiliximab), corticosteroids, anti-thymocyte globulins(ATG). Kindel et al. narrated that the development of eosinophilic oesophagitis may be a marker for the development of PTLD.Gajarski et al. concluded that Post-transplant Immunosuppressive induction therapy with cytolytic drugs (e.g OKT3 monoclonal antibody, ATG, thymoglobulin Basiliximab and daclizumab) , lowers the rate of PTLD, graft rejections, and early infections in post-transplant patients as compared patients who did not receive induction therapy . This depends upon the type of induction e.g OKT3 monoclonal antibody was associated with increased PTLDs and graft rejection, while Thymoglobulin/IL-2R antagonists demonstrated to decrease both the outcomes. Claire et al. described that overall mortality is decreasing due to the ongoing better understanding of pathophysiology and treatment options related to solid organ transplant. The mortality of the post-transplant congenital heart disease group was higher as compared to the cardiomyopathy group due to high comorbidities and surgical complications. The study by Christopher et al. showed that EBV seronegativity before transplant is associated with an increased risk of PTLD. PTLD is associated with lower survival rates as compared to non-PTLD groups.
Conclusion:
Our review illustrates that pretransplant seronegativity, OKT3 monoclonal antibody, and the development of eosinophilic esophagitis during the immunosuppressive regime increase the risk of PTLD. This study demonstrates that with a better understanding of PTLD and tumor behavior, the all-cause mortality rates are falling significantly. PTLD is one of the leading causes of mortality in post-transplant patients. However, the immunosuppressive induction therapy, absence of eosinophilic esophagitis, thymoglobulin/IL-2R antagonists improve survival and outcomes in the post-transplant patient in terms of graft rejection, graft failure, and development of PTLD.
Anwer:Incyte, Seattle Genetics, Acetylon Pharmaceuticals, AbbVie Pharma, Astellas Pharma, Celegene, Millennium Pharmaceuticals.: Honoraria, Research Funding, Speakers Bureau.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal